Claviculafractuur
Traumamechanisme
Val op de uitgestrekte hand of op de schouder, direct of indirect letsel.
Klinische presentatie
Pijn, zwelling, hematoom, afwijkende stand, crepiteren, drukpijn AC-gewricht. Beoordeel of huid bedreigd is. Onderzoek ook de thorax op mogelijke ribfracturen of hematopneumothorax. Sluit neurovasculair letsel en schouder- en scapulafracturen uit.
Aanvullend onderzoek
X-clavicula in AP- en 15-30 graden tilt craniaalwaartse richting1-3, op indicatie ook X-schouder of scapula. Overweeg bij mediale fractuur een CT-scan.
Classificatie
Classificatie volgens Robinson:
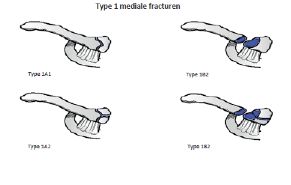
Type 1: 1/5 mediale deel clavicula
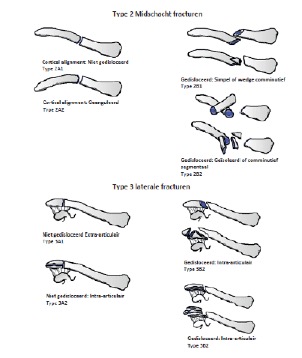
Type 2: tussenliggende 3/5 deel clavicula = Midschacht
Type3: 1/5 Laterale deel clavicula
Subdivisie voor mediale en laterale fracturen:
Groep A Niet-gedisloceerd
– A1 Extra-articulair
– A2 Intra-articulair
Groep B Gedisloceerd (= meer dan schachtbreedte dislocatie)
– B1 Extra-articulair
– B2 Intra-articulair
Subdivisie midschacht fracturen:
Groep A: Cortical Alignment
A1: Niet-gedisloceerd
A2: Geanguleerd
Groep B: Gedisloceerd (=meer dan schachtbreedte dislocatie)
B1: Simpel of comminutief wedge
B2: Geisoleerd of comminutief segmentaal
Conservatieve behandeling
Indicatie: Robinson 2A en 3A fracturen. Bij fracturen met verkorting en grote dislocatie van de fractuur fragmenten kan osteosynthese overwogen worden. Ongeveer 5-10% van de conservatief behandelde claviculafracturen eindigt in nonunion 4,5
Therapie:
Doel: pijncontrole en relatieve immobilisatie thv fractuur site met sling of ranselverband6. Adequate pijnstilling. Slingeroefeningen bij afname van pijn (doorgaans na 1 week). Uitbreiden mobiliseren indien pijnklachten dit toe laten. Belasting opbouwen na 6 weken en op geleide van de pijn
Deze fracturen worden in veel centra na behandeld volgens de VFC app en dan dus zonder standaard controles.
Alternatief kan nog onderstaand schema gebruikt worden.
Nabehandeling en controles:
1 week : functie, X-schouder voor bepalen of er secundaire dislocatie is opgetreden, oefen instructies, eventueel fysiotherapie
6 weken : X, functie
Bij twijfel na 6 weken over de genezing kan een follow up afspraak worden gemaakt op verzoek van patiënt of behandelaar. Complicaties: mal- of nonunion, vaat-/zenuwletsel, huidperforatie, pneumothorax, posttraumatische arthrose AC bij malunion of intra-articulaire fractuur, functionele pseudartrose en delayed union.
Operatieve behandeling
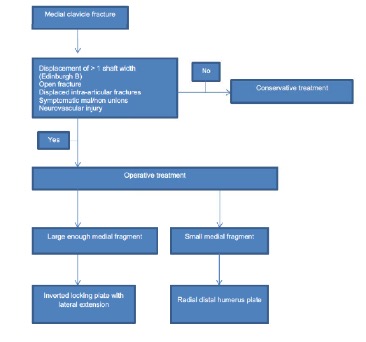
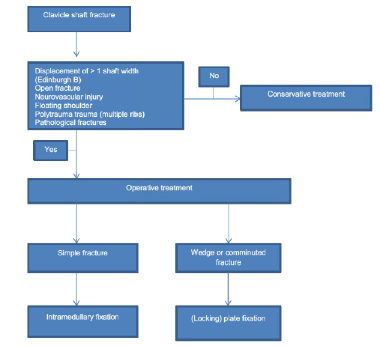
Indicatie: open fractuur, dreigende perforatie, ketenletsel van arm/schoudergordel (de “floating shoulder”), neurovasculaire bedreiging. Een fractuur bij een topsporter is een relatieve indicatie. Overweeg osteosynthese bij Robinson 1B, 2B en 3B fracturen; gedisloceerde fracturen of eventueel uitgesteld, wanneer fractuur bij X-controle na 1 week verder disloceert. Meerdere studies hebben laten zien dat er een lagere nonunion rate is bij operatieve behandeling en dat er een trend is richting slechtere functionele uitkomsten door conservatieve behandeling. Verkorting en dislocatie verhogen de kans op een nonunion. 7-13
Therapie: Osteosynthese
Er zijn meerdere opties, de meest gangbare osteosynthese is plaatosteosynthese voor midschacht en laterale claviculafracturen. Fixatie middels intramedullaire titanium elastic nail (TEN) is ook mogelijk alleen worden daar meer hardware related problems van gezien en alleen bij simpele midschacht fracturen 14-16. Meerdere studies hebben laten zien dat functioneel herstel tussen plaatosteosynthese en intramedulaire penfixatie vergelijkbaar is maar dat er een groot percentage van patienten klaagt over irritatie van het (met name intramedullaire) materiaal wat een tweede operatie noodzaakt 16,17. Er is enig bewijs dat behandeling van gedisloceerde mediale claviculafracturen met plaatosteosynthese kan geschieden. 18
Nabehandeling en controles: mobiliseren op geleide van de klachten.
Oefenstabiel, maar 6 weken onbelast.
1-2 week: mobiliseren op geleide van de pijn, geen belasting met aangedane zijde, evt fysiotherapie, postoperatieve foto indien nog niet gemaakt.
6 weken : X, indien klinisch weinig pijn bij deze controle kan belasting worden opgebouwd op geleide van pijnklachten
12 weken : X op indicatie, schouderfunctie dient volledig te zijn.
Complicaties: letsel van n. supraclavicularis, nonunion, nabloeding, wondinfectie, refractuur na verwijderen materiaal, breuk materiaal, uitbreken schroeven, osteomyelitis. Daarnaast vaat-/zenuwletsel (hematoom), pneumothorax, frozen shoulder, persisterende pijnklachten, last van materiaal 17-19
Bespreek met de patient de verschillende voor- en tegens van de behandelingen. Shared decision making is belangrijk om met patiënt een gedegen keuze te maken ten aanzien van de behandeling. Bespreek dus met de patiënt de complicaties van een conservatieve behandeling (mal- of nonunion, vaat-/zenuwletsel, huidperforatie, posttraumatische arthrose AC bij malunion of intra-articulaire fractuur, functionele pseudartrose en delayed union) als een operatieve behandeling (wondinfectie (3%), neurovasculair letsel (2%), hardware failure (1%), AC-luxatie (5%)). Schakel eventueel een keuzehulp in. (www.keuzehulp.info)
Midschacht claviculafractuur
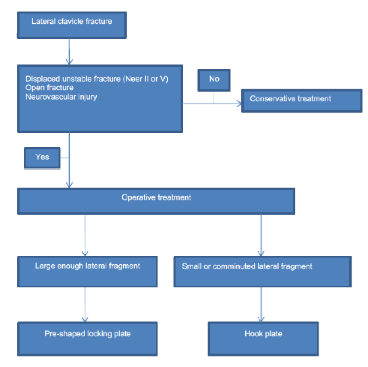
Laterale claviculafractuur
2. Omid R, Kidd C, Yi A, Villacis D, White E (2016) Measurement of Clavicle Fracture Shortening Using Computed Tomography and Chest Radiography. Clin Orthop Surg 8(4):367-372.
3. Austin L, O’Brien M, Zmistowski B, Ricchetti E, Kraeutler M, Joshi A, Fenlin JJ (2012) Additional x-ray views increase decision to treat clavicular fractures surgically. J Shoulder Elbow Surg 10:1263-1268.4.Fuglesang HF, Flugsrud GB, Randsborg PH, Stavem K, Utvag SE: Radiological and functional outcomes 2.7 years following conservatively treated completely displace midshaft clavicle fractures. Arch Orthop Trauma Surg 2016;136:17-25.
5.Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539.
6. DJC van der Ven, TK Timmers, PE Flikweert, ALS van Ijseldijk, G.D.J. van Olden. Plate fixation versus conservative treatment of displaced midshaft clavicle fractures: Functional outcome and patients’ satisfaction during a mean follow-up of 5 years; Injury. 2015 Nov;46(11):2223-9. doi: 10.1016/j.injury.2015.08.004. Epub 2015 Aug 10.
7.McKee RC, Whelan DB, Schemitsch EH, McKee MD: Operative versus nonoperative care of displaced midshaft clavicular fractures: A meta-analysis of randomized
8.Devji T, Kleinlugtenbelt Y, Evaniew N, Ristevski B, Khoudigian S, Bhandari M: Operative versus nonoperative interventions for common fractures of the clavicle: A meta-analysis of randomized controlled trials. CMAJ Open 2015;3: E396-E405.
9. Xu J, Xu L, Xu W, Gu Y, Xu J: Operative versus nonoperative treatment in the management of midshaft clavicular fractures: A meta-analysis of randomized controlled trials. J Shoulder Elbow Surg 2014;23:173-181.
10. Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE: Estimating the risk of nonunion following nonoperative treatment of a clavicular
fracture. J Bone Joint Surg Am 2004;86-A: 1359-1365.
11. Murray IR, Foster CJ, Eros A, Robinson CM: Risk factors for nonunion after nonoperative treatment of displaced midshaft fractures of the clavicle. J Bone Joint Surg Am 2013;95:1153-1158.
12. Woltz S, Krijnen P, Schipper IB. Plate fixation versus nonoperative treatment for displaced midshaft clavicular fractures: a meta-analysis of randomized controlled trials. J Bone Joint Surg Am 2017;99(12):1051-57
13. Woltz S, Sengab A, Krijnen P, Schipper IB. Does clavicular shortening after nonoperative treatment of midshaft fractures affect shoulder function? A systematic review. Arch Orthop Trauma Surg 2017 Aug;137(8):1047-53.
14. van der Meijden OA, Houwert RM, Hulsmans M, et al: Operative treatment of dislocated midshaft clavicular fractures: plate or intramedullary nail fixation? A randomized controlled trial. J Bone Joint Surg Am 2015;97:613-619.
15. Andrade-Silva FB, Kojima KE, Joeris A, Santos Silva J, Mattar R Jr: Single superiorly placed reconstruction plate compared with flexible intramedullary nailing for midshaft clavicular fractures: A prospective, randomized controlled trial. J Bone Joint Surg Am 2015;97:620-626
16. Hulsmans MH, van Heijl M, Houwert RM, et al: High irritation and removal rates after plate or nail fixation in patients with displaced midshaft clavicle fractures. Clin Orthop Rel Res 2017;475:532-539.
17. Houwert RM, Smeeing DP, Ahmed Ali U, Hietbrink F, Kruyt MC, van der Meijden OA: Plate fixation or intramedullary fixation for midshaft clavicle fractures: A systematic review and meta-analysis of randomized controlled trials and observational studies. J Shoulder Elbow Surg 2016;25:1195-1203.
18. Frima H, Houwert RM, Sommer C; Displaced medial clavicle fractures: operative treatment with locking compression plate fixation. Eur J Trauma Emerg Surg. 2020 Feb;46(1):207-213 19. Czajka CM, Kay A, Gary JL, et al: Symptomatic implant removal following dual mini-fragment plating for clavicular shaft fractures. J Orthop Trauma 2017;31: 236-240.
20. Leroux T, Wasserstein D, Henry P, et al: Rate of and risk factors for reoperations after open reduction and internal fixation of midshaft clavicle fractures: A populationbased study in Ontario, Canada. J Bone Joint Surg Am 2014;96:1119-1125.
21. Naimark M, Dufka FL, Han R, et al: Plate fixation of midshaft clavicular fractures: Patient-reported outcomes and hardwarerelated
complications. J Shoulder Elbow Surg 2016;25:739-746.
22 Frima H, van Heijl M, Michelitsch C, van der Meijden O, Beeres FJP, Houwert RM, Sommer C.Frima H, et al. Eur J Trauma Emerg Surg. 2020 Jun;46(3):519-529. doi: 10.1007/s00068-019-01122-4. Epub 2019 Apr 3.Eur J Trauma Emerg Surg. 2020. PMID: 30944950 Review.