Capitale MC (luxatie) fracturen
Algemene tekst
Intra-articulaire fracturen waarbij het caput os metacarpale betrokken is, komen relatief weinig voor en zijn in een groot deel van de gevallen comminutief. Ondanks blijvende, kleine, articulaire defecten kan het MCP-gewricht soms goed en pijnvrij functioneren.
Zie ook de landelijke richtlijn:
https://richtlijnendatabase.nl/richtlijn/handfracturen/fracturen_van_de_mcp-gewrichten.html
en
https://richtlijnendatabase.nl/richtlijn/handfracturen/fracturen_van_de_metacarpalia.html
Traumamechanisme
Veelal als gevolg van een vuistslag. Cave: bij open fractuur als gevolg van vuistslag tegen tanden, groot risico op diepe infectie!
Klinische presentatie
Zwelling, pijn en functio laesa over aangedane MCP.
Aanvullend onderzoek
X: AP, ware laterale van de desbetreffende MCP en oblique opname met hand in pronatie.
Laagdrempelig CT.
Er is geen bruikbare classificatie. Het gaat om mate van dislocatie en mate van communitie.
Conservatieve behandeling
Indicaties:
stabiel / anatomisch.
Immobiliseer capitale MC II tm V fracturen, die niet-operatief behandeld worden, gedurende 2 tot 3 weken met het MCP-gewricht in 50 tot 70° flexie en de IP-gewrichten vrij, en start daarna met actieve mobilisatie in een extensieblokkerende spalk.
Immobiliseer capitale MC I fracturen en/of doorgemaakte luxatie van het MCP1-gewricht, ongeacht de therapie, bij voorkeur met het MCP1-gewricht in 30° flexie, het CMC1-gewricht in een functionele positie en het IP1-gewricht vrij.
Nabehandeling en controles:
1 week :X-controle.
2-3 weken :X-controle, gips af en start handtherapie.
Complicaties: rotatie, secundaire dislocatie, stijfheid t.g.v. extensorpeesadhesies, collaterale ligamentaire contracturen en of dorsale kapselcontracturen.
Operatieve behandeling
Indicatie:
elke verplaatste fractuur >2mm, comminutieve, open fracturen.
Intra-articualire luxatie fracturen zijn meestal niet gesloten te reponeren.
Therapie:
Open repositie en interne fixatie (o.a. Headless compression Screw (Zie AO-Surgery Reference), plaatfixatie) dorsale benadering door het midden van de strekpees of door een sagitale band waarna deze hersteld dient te worden.
Nabehandeling en controles:
Bij comminutieve fracturen is ORIF lastig, soms onmogelijk, waardoor K-draad fixatie aangewezen is of ligamentotaxis.
Evt. rust, spalk voor 1 week, daarna oefentherapie (fysiotherapie/handtherapie).
1 week X, 3, 6 en 12 weken functiecontrole.
Verwijderen osteosynthesemateriaal op indicatie.
Complicaties:
infecties (m.n. bij fractuur als gevolg van vuistslag tegen tanden), functiebeperking, (osteonecrose), malunion, artrose.
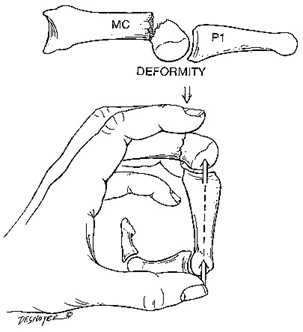
Jahhs Manoevre
- Martinez-Catalan N, Pajares S, Llanos L, Mahillo I, Calvo E. A Prospective Randomized Trial Comparing the Functional Results of Buddy Taping Versus Closed Reduction and Cast Immobilization in Patients With Fifth Metacarpal Neck Fractures. J Hand Surg Am. 2020.
- van Aaken J, Fusetti C, Luchina S, et al. Fifth metacarpal neck fractures treated with soft wrap/buddy taping compared to reduction and casting: results of a prospective, multicenter, randomized trial. Arch Orthop Trauma Surg. 2016;136(1):135-142.
- Pellatt R, Fomin I, Pienaar C, et al. Is Buddy Taping as Effective as Plaster Immobilization for Adults With an Uncomplicated Neck of Fifth Metacarpal Fracture? A Randomized Controlled Trial. Ann Emerg Med. 2019;74(1):88-97.
- Nederlandse richtlijn Handfracturen. 2018.